“Any medical student or surgical trainee will benefit from reading the relevant chapter before an attachment to one of these surgical specialties.”

Derek Alderson MD FRCS
President, Royal College of Surgeons of England
“This wonderful new book will be enormously useful to all undergraduates in Surgery. It has been produced in collaboration with students which has ensured that their need to demystify surgical procedures has been at the heart of the development.”

Miss Philippa Tostevin
Reader in Surgical Education and Head of the Centre of Clinical Education
St. George’s University of London

Stella Harris
Final Year Medical Student
University of Sydney

Imogen Thomson
Final Year Medical Student
University of Sydney

Alexander Jackson BMedSci (Hons) MBChB
Anaesthetics Registrar
University Hospital Southampton

Dermot Burke FRCS
Associate Professor in Surgery
Leeds Teaching Hospitals

Professor Simon Kay OBE FRCS
Consultant Plastic Surgeon and Lead for Hand Transplantation UK

Simon Patterson-Brown
Consultant General and Upper GI Surgeon, Edinburgh Royal Infirmar
Honorary Senior Lecturer, University of Edinburgh.
The Unofficial Guide to Surgery is the 12th book in the Unofficial Guide to Medicine Series, selling over 60,000 books. It is a concise summary of 120 of the most common and important operations across all surgical specialities, detailing how the operation is performed, indications, contraindications, complications, the pre/post-op care and follow up.
10 step operation guide across all common specialities
Illustrated core anatomy
Indications and contraindications
Answers to surgeon’s favourite questions
The Unofficial Guide to Surgery: Core Operations is a practical guide to common surgical operations, and it would be a useful resource for any medical or nursing student undertaking a rotation in surgery. Whether you’re a surgeon-to-be at the cutting edge of your cohort and hoping to wow your senior colleagues, or a budding psychiatrist unexcited about standing in theatre for hours on end, this textbook has something for you. It is detailed enough to serve as a study resource for the Christina Yangs of tomorrow, but organised and concise so that even the least surgically inclined student can feel more prepared for their obligatory stint in theatre after reading through an operation report while changing into their scrubs.
The textbook features an introduction to the principles of surgery, followed by detailed operation reports for an extensive array of common procedures, organised in chapters based on speciality. Helpfully, each operation report includes the definition of the procedure being performed, its indications, high-quality illustrations of relevant anatomy, a step-by-step guide to the procedure at a level appropriate for students and junior doctors, and interesting trivia on the operation or associated condition. Students will be prepared for a niche question from even the most esoteric consultant!
Core Topics
- Useful Theatre knowledge
- Upper Gastrointestinal
- Lower Gastrointestinal
- Breast
- Ear Nose and Throat
- Endocrine
- Vascular
- Urology
- Cardiothoracic
- Neurosurgery
- Orthopaedics
- Paediatrics
- Obstetrics and Gynaecology
- Interventional Radiology
- Ophthalmology
- Plastics

Katrina Mason
BSc (Hons) MBChB MRCS (ENT)
Chief Editor
A student enters theatre, and it is easy to forget that they may be seeing a surgical procedure for the first time. This entails seeing living, functioning organs working within a body before your very eyes, and it can be an overwhelming and humbling experience. You will not be the only one who has passed out in theatre. You will not be the only one who suddenly freezes when asked a difficult question. … What we have tried to do in this book is give safe and clear guidance on how to perform common surgical procedures. Remember, variations are based not only on the unit you might work in, but also your own personal preferences. The most important thing is to understand the principles behind the procedures and to be comfortable to perform them safely. There is also no substitute for clinical experience, so scrub in as often as you can, and let the words of this book come to life in the operating room.
Good luck with any upcoming exams. I look forward to calling you my colleague one day, should surgery be your passion.
Caesarean Section
Jenny Robertson and Katrina Mason
Definition
Delivery of the foetus through an incision in the lower abdomen and uterus.
Anaesthesia: regional or general.
Position: supine with left tilt to reduce aorto-caval compression.
Considerations: Prior to surgery, a urinary catheter is inserted to drain the bladder.
- A 10–15-cm-long transverse ‘Pfannenstiel’ or ‘Joel- Cohen’ incision is made 2–3 cm above the pubic symphysis, and subcutaneous fat is dissected using sharp or blunt dissection with bipolar diathermy for haemostasis.
- The rectus sheath is incised bilaterally for the full length of the incision. The sheath is then separated from the underlying rectus muscles by sharp and blunt dissection.
- The rectus muscles are then separated in the midline, exposing the peritoneum.
- Once intra-abdominal, the loose peritoneum over the lower segment is opened and the bladder is pushed down and protected with a Doyen’s retractor.
- Using a scalpel, a small transverse incision is made along the lower uterine segment of the uterus until the uterine cavity is entered or membranes are seen.
- The baby should be delivered with minimal delay by applying firm fundal pressure (only if cephalic lie). Once delivered, the cord is clamped in two places and divided. The baby can then be passed to the midwife or paediatric team.
- Syntocinon is then administered to enhance uterine contractions and expulsion of the placenta (unless
contraindicated) while gentle traction is applied to the cord. - Once the placenta is delivered, the uterus should be explored and cleaned to ensure that there is no retained placental tissue. The fallopian tubes and ovaries are inspected for any undiagnosed pathology, and the bladder is carefully inspected for any damage. The para-colic gutters are cleared of clots.
- Clamps are placed at the angles of the uterine incision, then the uterus is closed in two layers of running and/or interlocking dissolving sutures, ensuring haemostasis.
- The rectus sheath is closed with a running suture, then the skin is closed with subcutaneous non-absorbable sutures or staples.
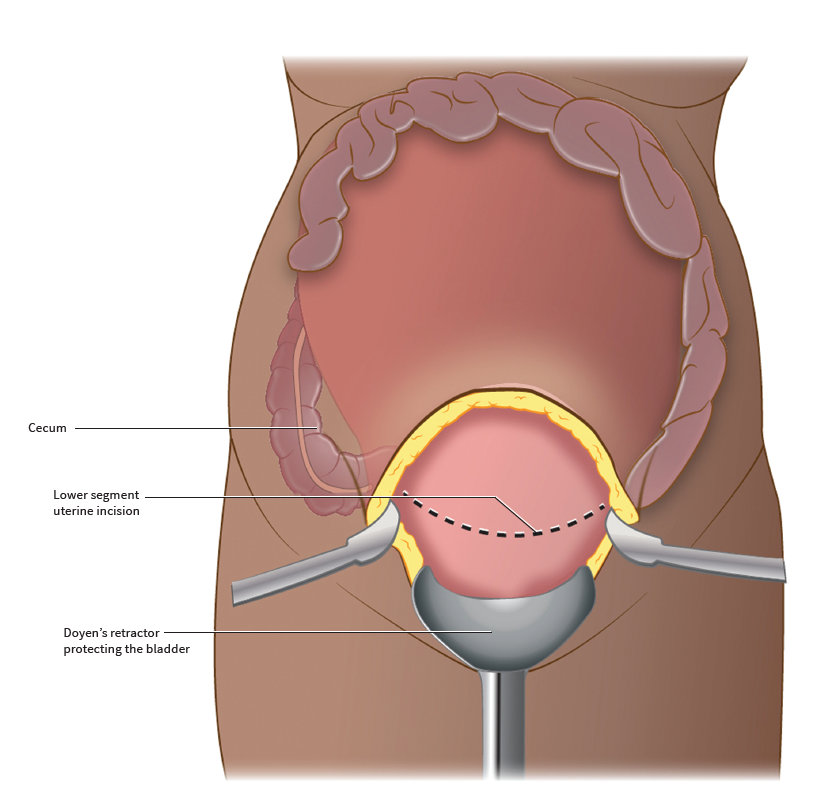
Figure 13.8 Exposure and incision of the uterus during a Caesarean Section
Gross Anatomy
consists of three layers of smooth muscle.
Neurovasculature
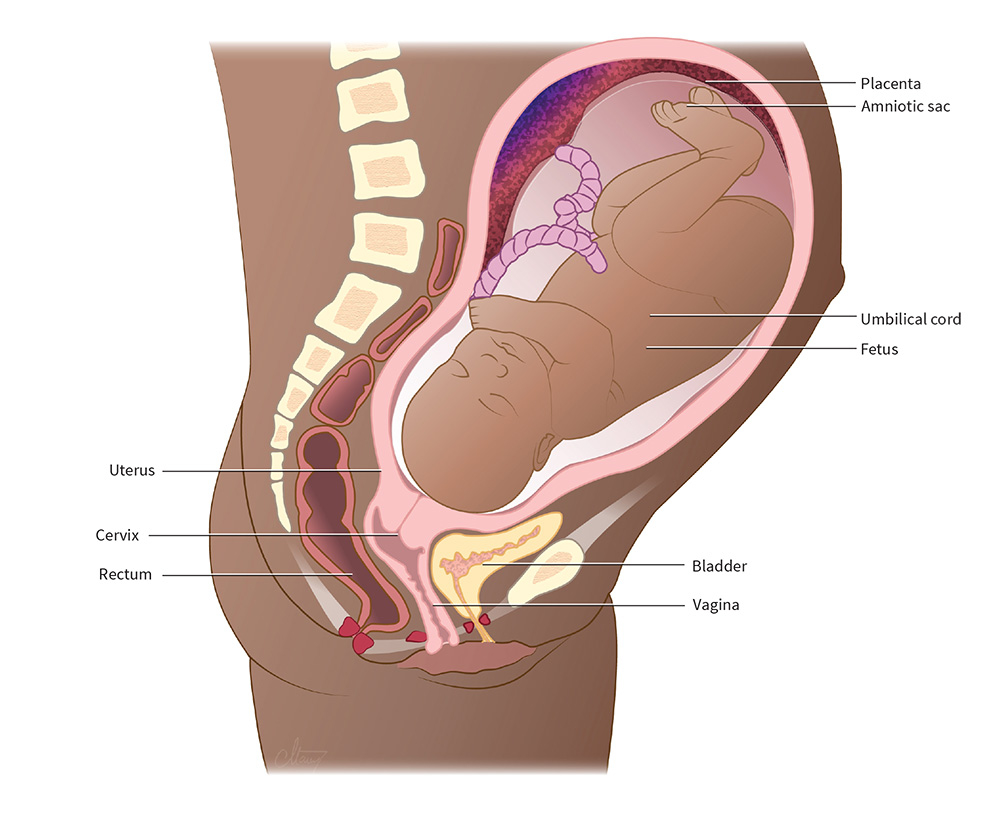
Figure 13.7 The full term gravid uterus
Indications
Caesarean sections can be performed for either maternal or foetal indications and may be planned elective or emergency procedures.
Elective
Emergency
ContraIndications
Early
Intermediate and Late
Inpatient
Outpatient
Surgeon’s Favourite Question
Why is the uterine incision made transversely wherever possible?
A transverse incision in the lower segment of the uterus heals better than a vertical incision, ruptures less frequently, and is less dangerous to make, as the placenta is less likely to be damaged because it is normally positioned antero-superiorly.
Contact Us
Are you a medical trainee, a student, a doctor or medical professional?
We’d love to hear from you for feedback or if you would like to contribute towards the Unoffical Guide to Medicine series.